Minimally Invasive Cardiac Surgery in Delhi
Minimally invasive cardiac surgery (MICS) is heart surgery performed through small incisions between the ribs, without splitting the full breastbone. It is used for valve repair and replacement, coronary bypass, ASD closure, and more. Most patients spend 3 to 5 days in the hospital and return to normal activity within 2 to 4 weeks. Not every patient is suitable. Candidacy depends on the heart condition being treated, anatomy, and overall health.
Minimally invasive cardiac surgery now accounts for roughly one-third of all cardiac surgeries performed globally. It has become a mainstream part of cardiac surgical practice rather than an experimental alternative.
Dr. Dinesh Kumar Mittal, Director and Head of Cardiothoracic and Vascular Surgery at Fortis Hospital, Shalimar Bagh, Delhi, provides specialist evaluation and surgical management across the full range of minimally invasive cardiac procedures.
Request a Consultation
What Is Minimally Invasive Cardiac Surgery?
Minimally invasive cardiac surgery (MICS) is heart surgery performed through one or more small incisions on the side or upper part of the chest, between the ribs, without fully cutting through the breastbone (sternum). Surgeons use specialised instruments, cameras, or robotic assistance to reach the heart. It covers a broad range of procedures, including valve repair, coronary bypass, and congenital heart defect correction.
In standard open-heart surgery, the surgeon makes a long incision down the front of the chest and separates the breastbone entirely to reach the heart. This gives excellent access but causes significant trauma to the chest wall, a lengthy healing process for the bone, and a recovery period of 6 to 8 weeks or longer before the patient can return to normal activities.
Minimally invasive approaches avoid this by working through smaller openings. The incisions are made between the ribs on the right side of the chest, or through only a partial cut in the upper sternum. Since the breastbone is either untouched or only partially divided, the chest wall heals much faster.
There are different levels of “minimally invasive.” Some approaches use video cameras and long instruments through small ports. Others use robotic arms controlled by the surgeon from a console. The right approach depends entirely on the procedure being performed and the patient’s anatomy.
What Conditions Can Be Treated with Minimally Invasive Cardiac Surgery?
Minimally invasive techniques are not limited to one type of heart problem. A wide range of adult cardiac conditions can be addressed through these approaches, provided the patient is a suitable candidate.
- Valve disease: It is the most common application. Mitral valve repair is the procedure most widely performed through a minimally invasive approach, with excellent long-term results across low-, intermediate-, and high-risk patients. Heart valve repair surgery and mitral and aortic valve replacement can both be performed through mini-thoracotomy in selected patients, avoiding a full sternotomy.
- Coronary artery disease (CAD): Affecting one or two vessels can be treated with minimally invasive coronary bypass. This is performed as a MIDCAB (Minimally Invasive Direct Coronary Artery Bypass) or MICS CABG, depending on the number of vessels involved. Patients with coronary artery disease who are not suitable for full open coronary artery bypass grafting may be assessed for these alternatives.
- Atrial septal defects (ASD): ASD and other congenital heart conditions in adults are also commonly addressed through minimally invasive incisions. ASD repair through a small right thoracotomy avoids a full sternotomy in suitable candidates.
- Atrial fibrillation: It can be treated surgically through the Maze procedure, which is now performed through small keyhole incisions in many centres.
- Aortic surgery: Including selected aneurysm repairs, may also be approached through minimally invasive techniques in carefully chosen patients.
The key point is that not every heart condition is amenable to a minimally invasive approach. Candidacy depends on anatomy, the type and complexity of the lesion, and whether the surgeon has clear access to the area that needs to be repaired.
Types of Minimally Invasive Cardiac Surgery
Minimally invasive cardiac surgery includes advanced heart procedures performed through small incisions, helping patients benefit from faster recovery, less pain, and reduced hospital stay compared to traditional open-heart surgery. It is not a single technique. It describes a family of approaches that share a common principle: accessing the heart through smaller incisions than with a full median sternotomy. The right technique depends on which part of the heart needs treatment.
The main approaches currently used are:
- Mini-sternotomy (partial sternotomy): A 6 to 8 cm incision is made through only the upper or lower portion of the breastbone, leaving most of it intact. This approach is commonly used for aortic valve surgery. It gives the surgeon good access to the aortic root while reducing chest trauma significantly.
- Mini-thoracotomy (right mini-thoracotomy): A 4 to 6 cm incision is made between the ribs on the right side of the chest. No incision is made in the breastbone at all. This is the most widely used approach for minimally invasive mitral valve surgery and is also used for ASD closure and tricuspid valve procedures.
- MIDCAB (Minimally Invasive Direct Coronary Artery Bypass): A small incision is made between the ribs on the left side of the chest. The internal mammary artery (a vessel inside the chest wall) is used to bypass the blocked coronary artery, most commonly the left anterior descending artery. The heart continues beating during the procedure; no heart-lung machine is used. This is known as off-pump, or beating-heart, surgery.
- MICS CABG (McGinn technique): A more advanced form of minimally invasive bypass that can treat multiple coronary vessels through a 5 to 7 cm incision in the chest, without a full sternotomy. Data from over 1,000 MICS CABG cases show a conversion rate to sternotomy of less than 2%, confirming it as a reproducible and reliable technique in experienced hands.
- Video-assisted and robotic-assisted surgery: Tiny cameras (thoracoscopes) or robotic arms are passed through small port incisions alongside the main working incision. These provide magnified visualisation inside the chest and allow surgeons to perform intricate repairs with greater precision. AI-assisted robotic systems are increasingly integrated into these procedures, improving real-time decision-making during complex cases.
Who Is a Candidate for Minimally Invasive Cardiac Surgery?
Candidacy for minimally invasive cardiac surgery depends on the patient’s anatomy, the complexity of the repair, and whether any factors make a small-incision approach less safe than conventional surgery.
Patients who are typically good candidates include those with:
- Mitral or aortic valve disease (stenosis or regurgitation) requiring repair or replacement
- An isolated blockage in the left anterior descending artery suitable for MIDCAB
- Multi-vessel coronary disease where anatomy allows MICS CABG access
- An atrial septal defect (ASD) without other significant cardiac pathology
- A need for redo cardiac surgery, where previous breastbone surgery has created scar tissue that makes a repeat sternotomy riskier
- Conditions such as osteoporosis or poorly controlled diabetes increase the risk of poor sternal healing after open surgery
Patients who may not be suitable, and who are better served by open-heart surgery, include those with:
- Complex multi-vessel coronary artery disease requiring a large number of bypass grafts
- Severe obesity, which limits access and visibility through small incisions
- A previous thoracotomy on the right side, which may have created scar tissue in the chest
- Peripheral vascular disease affecting the femoral arteries, which are needed for the bypass circuit in many minimally invasive approaches
- Severe calcification of the mitral annulus or aorta that requires direct access
- Significant lung disease that makes one-lung ventilation (which supports some MICS approaches) unsafe
The candidacy assessment involves echocardiography, CT angiography, and a detailed review of the patient’s anatomy and risk profile. It is not a decision that can be made from a scan report alone. A direct consultation with a surgeon experienced in both open and minimally invasive techniques is the correct starting point.
How Is Minimally Invasive Cardiac Surgery Performed in Delhi?
The procedure is performed in a specialised cardiac operating theatre equipped with high-definition camera systems and dedicated MICS instruments. Here is what the process involves for a typical minimally invasive valve or bypass procedure:
Step 1: Pre-procedure Assessment
The patient undergoes a full cardiac evaluation, including echocardiogram, CT angiography, blood tests, lung function assessment, and ECG. This confirms the anatomy, rules out contraindications to the minimally invasive approach, and allows the surgical team to plan the exact incision and access route before the day of surgery.
Step 2: Anaesthesia and Positioning
General anaesthesia is administered. For most right-sided thoracotomy approaches (valve and ASD procedures), a double-lumen breathing tube is placed to temporarily deflate the right lung, giving the surgeon a clear view inside the chest. The patient is positioned on their back with the right side slightly elevated.
Step 3: Incision and Access
The surgeon makes a 4 to 6 cm incision between the ribs on the appropriate side of the chest. For bypass procedures (MIDCAB/MICS CABG), this is on the left side. For valve surgery, it is typically on the right side. No breastbone is cut. Small port incisions may be added for camera placement or retractor instruments.
Step 4: Establishing Circulation Support (Where Required)
Many minimally invasive valve procedures require the heart to be temporarily stopped, and a heart-lung machine (cardiopulmonary bypass circuit) is used to circulate blood during the repair. The cannulae (tubes connecting the patient to the circuit) are placed in the groin, through the femoral artery and vein, rather than directly through the chest. For MIDCAB and off-pump MICS CABG, the heart continues beating throughout, and no bypass machine is used.
Step 5: The Repair or Bypass
The surgeon performs the required procedure under direct vision or with video or robotic assistance. For valve surgery, this means repairing or replacing the affected valve using the same techniques as open surgery, but through the more limited access. For coronary bypass, it means connecting the internal mammary artery to the blocked coronary artery using fine sutures.
Step 6: Closure and Weaning
Once the repair is confirmed on transoesophageal echocardiography (a real-time ultrasound inside the oesophagus that gives the surgeon a clear view of the heart during the procedure), the heart-lung machine is weaned off, and the heart resumes normal function. The small chest incision is closed in layers. One or two drainage tubes may remain in place for a brief period to prevent fluid collection.
Step 7: Recovery
The patient is moved to the cardiac ICU for close monitoring. Drainage tubes and the breathing tube are typically removed within 24 hours in uncomplicated cases. Most patients transfer to the ward within 1 to 2 days.
Procedure duration varies depending on the complexity of the repair. Most minimally invasive valve or bypass procedures take between 2 and 6 hours under anaesthesia.
Recovery After Minimally Invasive Cardiac Surgery
Most patients undergoing minimally invasive cardiac surgery spend 3 to 5 days in the hospital, compared with 7 to 10 days following conventional open-heart surgery. They return to light activities within 2 to 3 weeks and to full normal function within 4 to 6 weeks, without the sternal precautions (restrictions on lifting and arm movements) that follow a full sternotomy.
Here is what recovery typically looks like:
In hospital (Days 1 to 5): Patients spend 1 to 2 days in the cardiac ICU with continuous monitoring. In uncomplicated cases, drainage tubes and the breathing tube are removed within 24 hours. Physiotherapy and breathing exercises begin early. Patients are transferred to the cardiac ward and are encouraged to mobilise as soon as possible.
At home (Weeks 1 to 3): The incision site on the side of the chest requires care, but there is no healing breastbone to manage. Most patients can return to light activities, including desk work, within 2 to 3 weeks. Driving is usually permitted once the patient is no longer on strong pain medication and can react safely, typically within 3 to 4 weeks.
Weeks 4 to 6: Most patients resume full normal activity, including moderate exercise, by week 4 to 6. This is considerably faster than the 6 to 8 week breastbone healing period associated with open sternotomy.
Longer term: Cardiac rehabilitation is recommended after minimally invasive procedures, just as it is after open surgery. This includes structured exercise, lifestyle guidance, and medication review. Regular follow-up appointments with the surgical team ensure that the repair or bypass is working as expected.
Post-operative care includes:
- Regular medications as prescribed (antiplatelet agents, blood pressure medications, or anticoagulants, depending on the procedure)
- Wound monitoring for signs of infection at the incision site
- Echocardiography follow-up to assess heart function and repair durability
- Lifestyle modifications: stopping smoking, blood pressure control, and a heart-healthy diet
Minimally Invasive vs Open-Heart Surgery: Key Differences
Minimally invasive and open-heart surgery are not competing approaches. They address the same conditions through different access routes. The choice between them depends on the patient’s anatomy, the complexity of the repair, and whether the minimally invasive approach can safely deliver the same quality of result.
| Feature | Minimally Invasive Surgery | Open-Heart Surgery (Sternotomy) |
|---|---|---|
| Incision | 3-7 cm between ribs | 20-25 cm down the front of the chest |
| Breastbone | Untouched or partially divided | Fully split and wired back together |
| Hospital stay | 3–5 days (typical) | 7–10 days (typical) |
| Return to activity | 2–4 weeks | 6–8 weeks |
| Blood transfusion rate | Lower | Higher |
| Infection risk | Lower (smaller wound) | Slightly higher (sternal wound) |
| Suitability | Selected patients | Broader patient group |
| Multi-vessel bypass | Possible with MICS CABG in selected cases | Standard approach for complex multi-vessel disease |
The key clinical distinction is that open surgery remains the standard and preferred approach for complex multi-vessel coronary artery disease, where many bypass grafts are needed, and complete revascularisation requires wider access. Minimally invasive bypass is most reliable for one to two-vessel disease in appropriate anatomy.
For valve surgery and ASD repair, the minimally invasive approach has become mainstream at high-volume centres and delivers equivalent long-term results to open surgery in the right patients.
The decision is always made after a full assessment of the individual case. There is no universally “better” approach, only the approach that is better for a specific patient’s heart.
Minimally Invasive Cardiac Surgery Cost in Delhi
The minimally invasive cardiac surgery cost in Delhi varies from ₹1,70,000 to ₹4,50,000, depending on the type of procedure, the complexity of the repair, and the hospital. As a general guide:
| Procedure | Approximate Cost (INR) | Approximate Cost (USD) |
|---|---|---|
| Minimally invasive mitral or aortic valve surgery | ₹2,70,000 – ₹4,50,000 | USD 3,250 – 5,420 |
| MIDCAB (single vessel coronary bypass) | ₹1,70,000 – ₹2,80,000 | USD 2,050 – 3,370 |
| MICS CABG (multi-vessel bypass) | ₹1,70,000 – ₹2,80,000 | USD 2,050 – 3,370 |
| ASD repair (minimally invasive) | ₹1,80,000 – ₹2,90,000 | USD 2,170 – 3,490 |
These are indicative ranges for private hospitals in Delhi.
Minimally invasive bypass surgery in India typically starts from approximately USD 3,250 for international patients, making it significantly more affordable than equivalent procedures in the UK, USA, or Gulf countries, where costs are typically three to five times higher.
Factors that affect the final cost include:
- The type and complexity of the procedure (single valve vs. double valve, number of bypasses)
- Whether a heart-lung bypass machine is used (on-pump vs. off-pump)
- Duration of ICU stay and overall hospital admission
- Pre-operative investigations (CT angiography, echocardiogram, blood tests)
- Surgeon’s fees and operating theatre charges
- Post-operative medications and follow-up care
Most private health insurance policies in India cover minimally invasive cardiac surgery under inpatient hospitalisation benefits when performed for a documented clinical indication. Cashless treatment is available at empanelled hospitals, including Fortis Shalimar Bagh, subject to policy terms. Patients are advised to confirm coverage before admission.
For a personalised cost estimate based on specific investigation reports and clinical assessment, a consultation with Dr. Dinesh Kumar Mittal might be the recommended first step. See the cost of heart surgery in Delhi page for a broader overview of procedure costs.
Why Choose India for Minimally Invasive Cardiac Surgery?
India has become one of the most sought-after destinations for minimally invasive cardiac surgery among international patients, and for good reason.
- Cost advantage: Minimally invasive cardiac procedures in India cost a fraction of what the same surgery costs in the UK, the USA, or the GCC, without compromising surgical technique or hospital standards.
- Surgical expertise: India’s top cardiothoracic surgeons have trained at the leading institutions in the country and abroad. MCh-qualified surgeons with international fellowships and large case volumes perform the full range of MICS procedures routinely.
- NABH-accredited facilities: Fortis Hospital, Shalimar Bagh, operates under NABH accreditation, with dedicated cardiac ICUs, advanced imaging, and modern operating theatres meeting international care standards.
- Remote pre-assessment: International patients can share echocardiogram reports, CT angiography, and medical history for remote evaluation before travelling. This allows surgical planning to be confirmed before arrival, reducing the overall stay in Delhi.
- Medical Visa (M Visa) support: The hospital provides invitation letters and step-by-step guidance for the Medical Visa process, ensuring timely approvals aligned with the treatment schedule.
- Dedicated international patient coordination: A single coordinator manages the full journey, from initial enquiry and medical record review through to admission, surgery, and post-discharge support.
- Typical travel plan for international patients: Most patients plan a 10 to 14 day stay in Delhi for a minimally invasive procedure: 3 to 5 days for hospitalisation and a further 5 to 7 days for post-discharge monitoring before being cleared to fly.
Why Patients Choose Dr. Dinesh Kumar Mittal for Minimally Invasive Cardiac Surgery in Delhi?
Minimally invasive cardiac surgery is technically demanding. The results depend not only on the incision being smaller, but on the surgeon’s ability to perform a complete, precise repair through that more limited access. Choosing a surgeon with the right training and volume for this work is the most important decision.
Patients across Delhi NCR consult Dr. Dinesh Kumar Mittal for minimally invasive cardiac surgery because of:
- MCh in Cardiothoracic Surgery, AIIMS New Delhi: India’s highest qualification for complex heart surgery, from the country’s premier medical institution.
- Fellowship in Endovascular Stenting, Milan, Italy: Advanced international training in catheter-based and minimally invasive techniques, strengthening his approach to complex cardiac interventions.
- 10,000+ Cardiac Surgeries Over 25+ Years: A case volume that spans routine to high-risk and emergency presentations, including adult and paediatric cardiac surgery.
- Full Range of MICS Capability: Expertise in minimally invasive valve repair and replacement, MIDCAB, congenital defect closure, and aortic procedures, allowing patients to be assessed for the least invasive approach appropriate for their condition.
- Pioneer of the Neonatal Cardiac Surgery Programme: Established the neonatal cardiac surgery programme at Max Hospital, Shalimar Bagh. This reflects a level of surgical precision that transfers directly to minimally invasive work in adults.
- Active Professional Memberships: Indian Association of Cardiovascular Thoracic Surgeons (IACTS), Indian Medical Association (IMA), and Delhi Medical Council (DMC).
His approach is straightforward: assess each patient fully, determine whether a minimally invasive technique can safely achieve the same quality of repair as open surgery, and proceed with the approach that gives the best outcome for that patient’s specific heart.
Book a Consultation for Minimally Invasive Cardiac Surgery in Delhi
Many heart conditions that once required open surgery can now be addressed through a much smaller incision, with a significantly shorter and more comfortable recovery. Still, not every patient is a candidate, and not every condition is suitable. The right starting point is a thorough clinical assessment.
During your consultation, Dr. Dinesh Kumar Mittal will provide:
- A detailed review of your symptoms, cardiac history, and existing reports
- Echocardiogram and CT angiography review to assess anatomy and suitability for minimally invasive access
- A clear explanation of whether a minimally invasive approach is appropriate for your condition
- A comparison of minimally invasive and open surgical options with honest discussion of risks and benefits for your specific case
- A personalised written cost estimate and recovery timeline
Early consultation allows more time for planning, a wider range of surgical options, and the best possible preparation for the procedure.
If you have been told you need heart surgery, or if you have been diagnosed with valve disease, coronary artery disease, or a congenital heart condition and want to understand whether minimally invasive surgery is an option, a specialist consultation is the most important step you can take.
Frequently Asked Questions
What is the success rate of minimally invasive cardiac surgery in India? expand_more
Minimally invasive cardiac surgery achieves success rates comparable to those of traditional open-heart surgery when performed in the right patients by experienced surgeons. For coronary bypass surgery, studies show ~96% survival at 8 years and excellent graft success rates. For valve procedures, large registries report very low mortality and complication rates across patient groups.
What are the risks and complications of minimally invasive cardiac surgery? expand_more
Risks are similar to open-heart surgery and may include bleeding, infection, stroke, arrhythmias, and anaesthesia-related complications. Overall, compared with traditional surgery, risks such as infection, prolonged ventilation, and blood transfusions are usually lower.
Is minimally invasive cardiac surgery in India safe? expand_more
Yes, minimally invasive cardiac surgery in India is considered safe and effective when performed by experienced cardiac surgeons in advanced centers. Leading hospitals follow international protocols, with outcomes comparable to global standards and lower complication rates in selected patients.
What are the advantages of minimally invasive cardiac surgery over open-heart surgery? expand_more
Minimally invasive cardiac surgery offers smaller incisions, less pain, reduced blood loss, lower infection risk, shorter hospital stay, and faster recovery compared to traditional open-heart surgery, making it a preferred option for eligible patients.
How do I book a consultation with Dr. Dinesh Kumar Mittal? expand_more
You can book an appointment with Dr. Dinesh Kumar Mittal by contacting Fortis Hospital, Shalimar Bagh directly or using their online appointment booking facility. International patients can also share medical reports, including echocardiogram and CT angiography, for a remote pre-assessment before travelling to Delhi.

Dr. Dinesh Kumar Mittal's Content Team
Dr. Dinesh Kumar Mittal's medical content team specialises in creating accurate, clear, and patient-focused healthcare content. With strong clinical understanding and expertise in technical writing and SEO, the team translates complex medical information into reliable, accessible resources that support informed decisions and uphold Dr. Mittal's commitment to quality care.
This content is reviewed by Dr. Dinesh Kumar Mittal
Related Treatments
Aneurysm Repair Surgery in Delhi
An aneurysm is a medical condition in which the walls of the blood vessels are weakened and bulged out. It…
Bentall Procedure in Delhi
Serious problems of the aorta and aortic valve can be life-threatening if not treated in time. The Bentall Procedure is a specialised,…
Atrial Septal Defect (ASD) Repair in Delhi
Every year, thousands of people confront the burden of living with an atrial septal defect (ASD), a hole in their…
Aortic and Mitral Valve Replacement Surgery in Delhi
Heart valve disease can quietly affect your daily life, causing breathlessness, fatigue, chest discomfort, or swelling. When medications are no…
Heart Valve Repair Surgery in Delhi – Dr. Dinesh Kumar Mittal
When your heart valves don’t work properly, it can affect how blood flows through your heart, leading to symptoms like…
Related Blogs
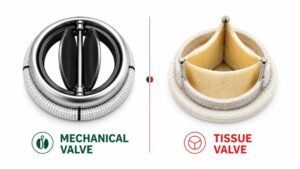
Mechanical vs Tissue Valve: Which Is Right for You?
Being told that you need a heart valve replacement often raises one question before any other: “Which…
Read Article →
Life After Heart Surgery: Recovery, Risks & What to Expect?
The surgery is done. The heart is beating. And now, sitting in a hospital ward…
Read Article →
What Causes a Hole in the Heart and How is it Treated?
The heart is the powerhouse of the entire body, pumping blood into every cell.…
Read Article →
Is Heart Valve Repair or Replacement a Major Surgery? – Dr. Dinesh Mittal
The aortic valve is one of four valves that control blood flow in the…
Read Article →
Aortic Valve Repair vs. Replacement: How Do They Differ?
Aortic valve repair and aortic valve replacement are two surgical procedures used to treat…
Read Article →